Gastrointestinal Surgical Training in Davos
This page records the origins, development, and long-term operation of the Davos gastrointestinal surgical training courses, with particular emphasis on the material, organisational, and practical aspects relevant to the author’s involvement.
Author context: Oscar Baldomero — anatomical preparation supporting hands-on gastrointestinal surgical training in Davos.
Contents
1 — Origins of the GI Training Concept
The concept of structured gastrointestinal surgical training in Davos emerged against the background of the established AO orthopaedic courses, which had demonstrated the effectiveness of hands-on, model-based teaching for operative skills. By the late 1970s, these courses had become a reference point for surgical education, emphasising repetition, standardisation, and direct engagement with anatomically realistic training material.
Martin Allgöwer, who played a central role in the development of the AO courses, recognised that comparable training opportunities did not exist for visceral surgery. He articulated a broader educational view in which skeletal (“bone”) and visceral (“belly”) surgery were understood as complementary domains requiring a shared anatomical and technical foundation. From this perspective, gastrointestinal surgery should be taught not solely through observation or apprenticeship, but through structured practical exercises comparable in rigor to those used in orthopaedics.
Early attempts to realise such a programme were limited by the absence of suitable training models. While the educational framework and surgical expertise were present, existing materials did not permit repeated practice of complex gastrointestinal procedures under realistic conditions. As a result, the idea of a gastrointestinal course remained largely conceptual for several years, despite sustained interest among surgeons involved in Davos-based teaching.
By the early 1980s, renewed efforts were made to establish a gastrointestinal training course that would parallel the orthopaedic model in both structure and ambition. This renewed interest was driven by the conviction that visceral surgical skills could be taught systematically if appropriate anatomical training material could be developed. The resolution of this problem, and the subsequent establishment of the Davos gastrointestinal courses, is addressed in the following sections.
2 — The Model Problem
Despite clear educational intent and sustained interest among surgeons involved in Davos-based teaching, early attempts to establish a structured gastrointestinal training course were constrained by a practical limitation: the absence of suitable anatomical training material. While orthopaedic courses could rely on solid models that permitted repeated handling and mechanical stress, no equivalent existed for visceral surgery that allowed realistic practice without reliance on live tissue or one-time use specimens.
Gastrointestinal procedures place specific demands on training material. Suturing, anastomosis, and dissection techniques require repeated manipulation of delicate structures under tension, with consistent tactile feedback and anatomical fidelity. Existing alternatives at the time—whether observation, apprenticeship, or occasional use of animal tissue— did not permit systematic repetition, comparison between trainees, or standardisation across courses. As a result, the educational framework envisaged by Martin Allgöwer could not be realised in practice.
This limitation was not one of surgical expertise or pedagogical design, but of material feasibility. Without training specimens that could be prepared reproducibly, handled repeatedly, and integrated into a structured course format, gastrointestinal surgery remained resistant to the kind of hands-on, model-based teaching that had proven effective in orthopaedics. The resolution of this problem required a different approach to anatomical preparation—one capable of bridging the gap between realism, durability, and repeatability.
It was this unresolved material constraint that delayed the implementation of gastrointestinal training in Davos for several years, and which ultimately prompted renewed efforts to identify or develop appropriate training specimens. How this problem was addressed, and how it led to the establishment of the Davos gastrointestinal courses, is the subject of the following section.

3 — Encounter and Re-activation
The impasse created by the lack of suitable gastrointestinal training material was resolved through a chance encounter rather than through a planned development programme. During the early 1980s, Martin Allgöwer encountered intestinal specimens that had been prepared by Oscar Baldomero while he was working at the Royal College of Surgeons in London. These specimens demonstrated that gastrointestinal tissue could be prepared in a way that allowed realistic handling, repeated manipulation, and consistent use in a teaching context.
The significance of this encounter lay not only in the quality of the specimens themselves, but in what they made possible. For the first time, the long-standing idea of a structured gastrointestinal training course could be matched with material that met the practical requirements of hands-on teaching. Following this encounter, Baldomero was invited to demonstrate the preparation and use of these specimens to a small group of surgeons. This demonstration showed that complex gastrointestinal procedures, including suturing and anastomosis, could be practised repeatedly under controlled and reproducible conditions.
This moment marked the re-activation of the gastrointestinal training concept in Davos. What had previously remained a theoretical aspiration was now technically feasible. The surgeons involved in these early demonstrations subsequently formed the core of the founding faculty of the Davos gastrointestinal courses and the associated course foundation. Baldomero’s contribution at this stage was practical and enabling: the provision and demonstration of training material that resolved the central obstacle identified in earlier attempts to establish the course.
The establishment of the Davos gastrointestinal training programme thus followed a clear sequence: educational intent, material limitation, and technical resolution. The subsequent development of the courses, including their structure, delivery, and long-term operation, built upon this initial re-activation and is described in the sections that follow.
4 — Establishment of the Davos GI Courses
Following the successful demonstration of anatomically prepared gastrointestinal specimens, the conditions were in place to move from feasibility to implementation. What had previously remained a conceptual ambition could now be realised as a structured training programme. The early demonstrations confirmed that complex gastrointestinal procedures could be practised repeatedly under controlled conditions, providing a practical foundation for course development.
On this basis, a gastrointestinal surgical training course was formally established in Davos during the mid-1980s. The course was modelled in part on the structure of the existing AO orthopaedic workshops, combining short theoretical introductions with extended hands-on practical exercises. Emphasis was placed on standardised techniques, repeatability, and direct engagement with anatomical material, allowing participants to acquire and refine operative skills through supervised practice.
A small group of surgeons who had participated in the initial demonstrations formed the core of the founding faculty. Together, they defined the course content, sequence of exercises, and instructional approach, ensuring consistency across teaching sessions. The availability of suitable training specimens was central to this process, as it allowed exercises to be designed around specific procedural objectives rather than adapted to material limitations.
As participation increased and the scope of the course expanded, organisational structures were formalised to support continuity and long-term development. This led to the establishment of a dedicated course foundation, providing an institutional framework for governance, faculty succession, and curriculum evolution. Within this framework, the Davos gastrointestinal courses developed into a recurring educational programme, capable of maintaining consistent standards while adapting to advances in surgical technique.
The establishment of the courses marked the transition from experimental demonstration to sustained surgical education. It provided a platform through which gastrointestinal surgical training could be delivered systematically, laying the groundwork for the later expansion, diversification, and long-term operation of the programme described in subsequent sections.
5 — Training Philosophy and Technique
The gastrointestinal courses in Davos were founded on the principle that operative competence is acquired through structured repetition under consistent conditions. Teaching was therefore organised around clearly defined procedural steps, allowing participants to practise techniques multiple times and to compare outcomes within a standardised framework. This approach mirrored the pedagogical logic of the AO orthopaedic courses, adapted to the specific demands of visceral surgery.
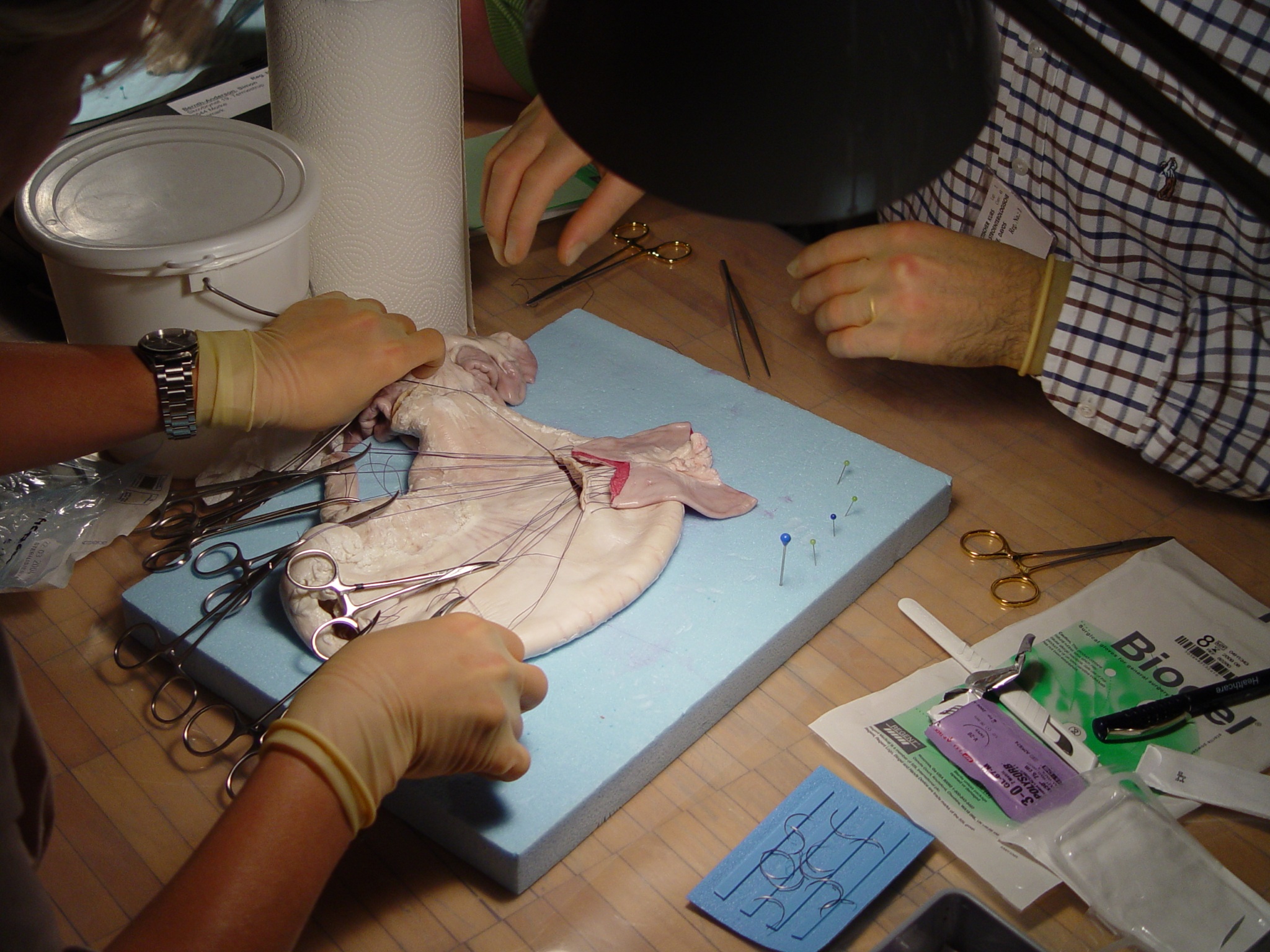
Particular emphasis was placed on suturing and anastomotic techniques. Exercises were designed to develop precision, economy of movement, and an understanding of tissue behaviour under tension. By working with anatomically prepared specimens that permitted realistic handling, participants could focus on technique rather than compensating for material limitations. This enabled instruction to move beyond demonstration toward active skill acquisition.
Over time, a shared instructional doctrine emerged, reflecting both anatomical principles and practical surgical requirements. This included agreement on sequence, hand positioning, needle handling, and suture placement, fostering a common technical language among instructors and participants. The aim was not to impose stylistic uniformity, but to establish reproducible methods that could be evaluated, refined, and taught consistently across courses and faculty.
The course structure encouraged direct interaction between instructors and participants, with close supervision during practical exercises and immediate feedback. This facilitated correction of technique at an early stage and supported incremental improvement over the duration of the course. In this way, the Davos gastrointestinal programme emphasised learning through doing, grounded in anatomical realism and reinforced by repeated practice within a coherent teaching framework.
6 — Expansion, Continuity, and Long-Term Involvement
Following their establishment, the Davos gastrointestinal courses expanded steadily in scope, participation, and technical breadth. Over subsequent decades, the programme evolved to incorporate new procedures and technologies, including advances in laparoscopic techniques and the use of stapling devices, while maintaining its emphasis on structured, hands-on training. Throughout this expansion, continuity of educational standards remained a central concern.
Oscar Baldomero remained involved with the gastrointestinal courses from the initial preparatory and pre-course sessions through their subsequent development and long-term operation, continuing in this role until his retirement in approximately 2022. His involvement extended beyond the founding phase and formed part of the practical infrastructure that supported the consistent delivery of the programme over time.
In addition to his early technical contributions, Baldomero assumed ongoing responsibility for organising the preparation of anatomical specimens used in the courses and for coordinating the delivery of appropriate training material for each specific exercise. This work was carried out with the assistance of small groups of medical students, typically numbering three, who participated in specimen preparation under his supervision. Ensuring that suitable specimens were available, prepared to a consistent standard, and aligned with the instructional sequence of the course was essential to maintaining its educational effectiveness.
This continuity of material preparation and logistical coordination allowed successive generations of instructors and participants to work within a stable training framework, even as surgical techniques and technologies evolved. In this way, the Davos gastrointestinal courses combined adaptability with consistency, enabling long-term institutional sustainability while remaining grounded in the original educational principles on which the programme had been founded.
Note: This page forms part of the historical documentation on balmed.ch. Additional source material can be listed on the Publications page as it is assembled.